
Cancer as a Metabolic Disease, by Thomas N. Seyfried
Browse on Amazon!
I have many reasons for wanting to read this book:
- non-hodgkins lymphoma
- merkel cell carcinoma
- breast cancer
- liver cancer
- pancreatic cancer
- bladder cancer
- lung cancer
- glioblastomas
- melanoma
- colon cancer
- more (sadly)
Some days it feels as if there isn’t a type of cancer that I’m either not related to or know by aquantance. This sad reality is not surprising. Seyfried notes that after more than 20 years of cancer research focused on the genetic model, more people are being diagnosed with cancer every year and, sadly, more people are dying of it. (12)
This is not just my reality, it is our shared reality. And it is why I consider this book an important treatise on the topic, even if I’m not a doctor.
Who should read this book?
Healthcare Professionals: Generally, if you are healthcare professional engaged in the context of cancer treatment, it is imperative that you read this book. This needs to be part of the discussion in the medical context, otherwise we very well may miss out on an approach to cancer treatment that targets cancer cells while promoting the health of “normal” cells. No other cancer therapy currently does this. Radiation is not selective, and neither are most chemotherapies. The rates of cancer mortality have not decreased in the last 20 years of refining our traditional approaches.
Cancer Patients: If you have cancer, you should read this book. You’ll have a better understanding of the fundamentals of the disease, the treatments you are undergoing, and possible options for your therapy that you may not have known about. The conversations you have with your doctors may even change as a result of reading this. Certainly your understanding will.
One huge disclaimer: Seyfried provides much needed information that you can use when evaluating your treatment options. What this isn’t, however, is a miracle cure. I find much of the coverage of cancer in the mainstream press to be infuriating because it promises false hope to those who are most desperate.
Cancer as a Metabolic Disease is not that type of book.
You’re going to work hard to get through it. You’re going to come out the other end with a better understanding of cancer. And you’re going to understand your treatment options in a new context. You may even discover some options you didn’t know existed. But at the end of the day, it’s science and not miracle. This is an important point to keep in mind.
Friends/family of cancer patients: While I think that anyone with a family member or friend with cancer should read this book, I say that with reservation. Far too often I see someone read a book on cancer that promises an unconventional “cure”, and then proceed to force the book (or approach, or ideology) on the person with cancer. So read the book if you want to understand cancer, its causes, the failure of current approaches, and possible alternative therapies…but please don’t push this as part of an agenda.
Low-carbers/Ketoers: If you’re interested in the science behind low carb diets, health and nutrition, this book will likely blow your mind. If you just prefer to be told what to do and what to eat, and could care less about the science behind low carb diets, this is really not the book for you.
Health-concious/longevity curious: There’s a growing community of people out there who are interested in understanding nutrition and it’s relationship to optimizing health and longevity. This is an excellent book for you. While its focus is mainly on cancer, Seyfried does an admirable job of looking at it in the context of optimal health and longevity.
The Premise of Cancer as a Metabolic Disease
Seyfried carefully articulates a fascinating theory: that cancer is not the result of genetic mutation (often referred to as the Somatic Mutation Theory), but is the result of metabolic dysregulation first articulated by Otto Warburg. Seyfreid repeats this as chorus throughout the book: “cancer is not a genetic disease, but is a metabolic disease involving mitochondrial dysfunction and respiratory insufficiency” (219).
I approached this idea with a great deal of skepticism, as I presumed that the root cause of cancer was settled (mutations in genes). After reading this book, I’m convinced that it’s not. The mutations that I have long assumed to be the causes of cancer, may very well be the result of impaired respiration.
Until we abandon the idea that cancer is a genetic disease and recognize that the mutations are downstream epiphenomina of the disease, there will be little progress in defeating cancer. (160).
Because this notion of genetic mutation as causative agent is so entrenched in both the lay-understanding and scientific understanding of cancer, Seyfried gives much attention to this explanation and its failings. Perhaps more than anything else, Seyfried’s examination of metastasis in the context of random genetic mutation drove home for me just how flawed the current theory is.
It is difficult to understand how a collection of gene mutations, many of which are random, could produce cells with the capacity to detach from the primary tumor, intravasate into the circulation and lymphatic systems, evade immune attack, extravasate at distant capillary beds, and recapitulate epithelial characteristics following invasion and proliferation in distant organs. This would be quite a feat for a cell with a disorganized genome. (217)
Metastasis is a highly orchestrated series of events that require a great deal of specializations for a cell to accomplish. The notion that these could result from random mutation seems ludicrous.
So What Causes Cancer?
If we entertain the idea that cancer is not caused by gene mutations, we are left with a fundamental question, “So what causes cancer?” Yes, Seyfried says it’s “impaired cellular metabolism”…but what causes that? And what causes the thing that causes that? And so we could go, round and round, dizzying ourselves with ever more nuanced explanations of the roles of glucose and glutamine metabolism, fermentation, respiration and mitochondrial dysfunction. But Seyfried is clear on this point: “Any unspecific condition that damages a cell’s respiratory capacity, but is not severe enough to kill the cell, can potentially initiate the path to a malignant cancer” (255). Exposure to radiation, chemicals, viruses and, of course, chronic inflammation (ala Alice and Fred Ottoboni) are all environmental factors that can initiate this (18). And of course, there are numerous genetic and epigenetic factors as well (91).
To understand this is to come face to face with a rather uncomfortable realization: The very tools we use to treat cancer – radiation and chemotherapy – are themselves promoters of inflammation and may, in fact, increase risk or even select for drug resistance. Take for example, this viscous cycle: Chemotherapy causes nausea. Nausea is treated with steroids. Steroids elevate serum glucose. Elevated glucose enhances tumor survival and drug resistance. (283)
This is our current “cure”.
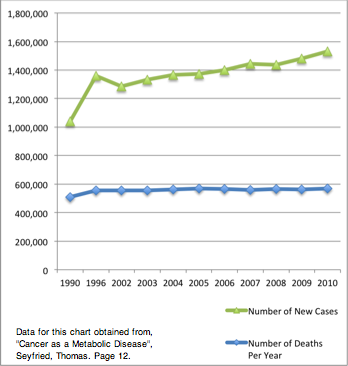
Twenty Years of “Progress” in Cancer Prevention and Treatment
Is it any wonder that after decades of pursuing such treatments, after years of investing in research that assumes cancer is the result of genetic mutation, we have witnessed year-over-year increases in new cases of cancer and no reduction in mortality? Consider the data charted to the right and ask yourself, “Are we making progress with our current theories and treatments?” Clearly not. But we’re throwing more and more money research based on a profoundly flawed understanding of the disease.
Can a low carbohydrate ketogenic diet cure cancer?
I’m really loathe to use the term “cure”, so I shan’t. There are far too many people promoting low carb as the cure all for everything that ails you, and I’d like to disabuse anyone of the notion that it’s going to cure cancer on its own. It’s a tool, and one that should be used in the greater context of treatment. Even Seyfried is clear: “…we do not believe that the [restricted ketogenic diet], used as a singular therapy, will provide complete disease resolution for most patients” (364). In fact, Seyfried writes of his research on mice that “the [ketogenic diet] had no therapeutic efficacy against tumor growth when consumed […] in unrestricted amounts” (295).
The key phrase being “unrestricted”. Seyfried is clear that a restricted ketogenic diet has its place in cancer treatment. His protocol is outlined in several phases:
Phase 1: Initiation – Pateints undertake a ketogenic diet and measure blood glucose and ketones regularly to ensure they are in therapeutic ranges. “Blood glucose ranges between 3.0 and 3.5 mM (55-65 mg/dl) and betahydroxybutyrate ranges between 4 and 7 mM should be effective for reducing tumor growth in most patients” (356).
What’s more, the ketogenic diet he refers to is not the one you may be utilizing. It’s an energy restricted ketogenic diet, one where the total caloric consumption is governed by the effect food choices and energy intake have on serum ketone and glucose readings. In other words, there’s not a specific, universally applicable caloric limit recommended for everyone. Instead, measure and adjust as necessary.
Phase 2: Surgery – After spending some time (several weeks) maintaining the ketone and glucose ranges recommended in Initiation above, “dietary energy reduction and the [ketogenic diet] will reduce tumor vascularization and inflammation and will more clearly delineate tumor tissue from the surrounding normal tissue” (363). This is the opportune time to excise the tumor.
Seyfried acknowledges that not all patients can wait for multiple weeks while the ketogenic diet reduces inflammation and vascularization. Conversely, “the urge to resect malignant tumors as soon as possible after diagnosis may not be in the best interests of all patients and could actually exacerbate disease progression by inducing inflammation in the microenvironment” (363). Clearly, determining when to operate will depend on the details and state of the disease at the time of diagnosis.
Phase 3: Maintenance – “The goal of the maintenance strategy is to increase the probability of survival for at least 36 months in patients with advanced metastatic cancer” (364). This phase of treatment is designed to extend life by maintaining metabolic pressure on cancer cells.
Seyfried advocates continuing to follow an energy restricted ketogenic diet, continued monitoring of serum glucose and ketone levels, and suggests utilizing a glucose and glutamine-targeting drug therapy of 2-DG (30-40mg/kg per day) and phenybutyrate (15g/day). 2-DG targets glucose metabolism and glycolosis. Phenylbutyrate helps lower circulating glutamine levels. Both glucose and glutamine are primary sources of energy in cancer cell metabolism. (364)
A word of caution: It is imperative that dosing and monitoring is done in consultation with a physician. This is not the domain for do-it-yourselfers, as improper dosing can have toxic effects.
Will a low carbohydrate ketogenic diet prevent cancer?
Perhaps.
We know that low carbohydrate ketogenic diets are anti-inflammatory and reduce C-RP. These are themselves preventative. Seyfried also describes how ketone metabolism reduces cancer risk (378) and the roles of energy restriction, fasting and cancer prevention. The theory behind the energy restriction and fasting is to prompt the (metabolically fragile) extant cancer cells to initiate autophagy and autolytic cannibalism. (383) He speculates that a 7 day fast performed once a year is the ideal cancer preventative, but that multiple shorter (2-3 day fasts) might have the same cancer-preventative effect. Additionally, “A ketogenic diet consumed for 1 week should also be an effective cancer-prevention strategy as long as the blood glucose and ketones are maintained within the therapeutic ranges” (383).
Is Seyfried right?
I’m a skeptical person by nature, and I approached Cancer as a Metabolic Disease with a great deal of doubt. Ultimately, I’m unqualified to adjudicate whether or not Seyfried’s hypothesis is correct. However, I’m swayed enough by his arguments that I want this to be part of the professional discourse until the scientists, researchers and practitioners can reach consensus on it. His credentials are impeccable and his book is meticulously, if not lovingly, written and referenced. He lays out his case in exquisite detail. If he is right, the ramifications are nearly beyond comprehension. Decades of research will have to be reinterpreted, standard therapies revised, and the profile of hope -something far too narrow and ephemeral for many cancer patients- will be reified and extended by Seyfried’s new praxis.
Thanks and acknowledgements
I would like to extend sincere thanks to Dr. Thomas Seyfried and Wiley publishing for endeavoring to provide me with a review copy of Cancer as a Metabolic Disease. I hope that my review contributes in some small way to the awareness of Seyfried’s theory of the causes of and treatments for cancer.
Many thanks, Michael, for your great review of Dr Seyfried’s pioneering work. You have done a superb job of communicating the sense of an extremely difficult but important treatise in an interesting and informative manner to those of us who do not have the time or perhaps even the background to tackle the book. We are sincerely grateful to you.
Not having actually read the book, we can only judge from your excellent review that Dr, Seyfried’s research has brought him to a truth (perhaps just to the threshold, but a truth never-the-less). A truth is a natural law that is absolute – like the law of gravity.
All aspects of the universe are governed by natural laws. This is true for all life forms as well as for the inanimate world. Fortunately, the creation of natural laws was not capricious or careless. Natural laws are not arbitrary. They are precise and predictable. Otherwise we would have chaos.
The truth that appears to be emerging in the findings of Dr. Seyfried (and other scientists in closely related fields) is that the fuel required for optimal operation of the human body is dictated by a natural law that describes the boundaries within which macronutrients and micronutrients are most advantageous. This natural law is the reason for the great benefits bestowed by the ketogenic diet. It fits what serves the human body best.
Numerous mechanisms by which nutritional indiscretions cause chronic inflammation have been demonstrated clinically and in the laboratory, and “Inflammation is now widely appreciated in the pathogenesis of many human diseases. These extend from the well-known inflammatory diseases such as arthritis and periodontal disease to those not previously linked to aberrant inflammation that today include diseases affecting many individuals such as cancer, cardiovascular diseases, asthma, and Alzheimer’s disease (1).
Dr. Seyfried’s finding that cancer is a metabolic disease applies equally to all of the current noninfectious chronic diseases we are now facing as epidemics. We do not have to search for new and novel biochemical pathways to explain obesity or diabetes. We just have to continue increasing our knowledge and understanding of the natural law of healthful nutrition.
Again, many thanks.
1.) Serhan CN. Lipoxins and aspirin-triggered 15-epi-lipoxins are the first lipid mediators of endogenous anti-inflammation and resolution. Prostaglandins, Leucotrienes and Essential Fatty Acids. 2005; 73: 141.
I heard of this book quite a while ago when I first listened to Prof Seyfried interviewed as part of a pod cast series on fasting and cancer prevention.
I msut thank Michael for this excellent and timely review. I absolutely agree that this book should be compulsory reading for healthcare staff and researchers invovled in treating cancer patients to engage in constructive discussions between the current traditional approach which might as flawed as our nutritional one and the not so new but hopefully emerging view of cancer as a metabolic disease. As a Paleofaster I have read extensively on the benefits of fasting and ketogenesis. Like Prof Seyfried however I do not think you can cure cancer via ketosis and starvation. Once cancer has started you have to kill the overproliferating cells with the more conventional treatments of chemo and radiation therapy and surgery where applicable. But again as Prof Seyfried advocates you can combine the dietary approach to aid the fight against cancer thus recognising the imporant metabolic component of this disease. On the other hand ketogenesis and prolonged fasting (doesn’t prof Seyfried advise for at least a once a year week long fast to rest the system and get rid of misbehaving mitochondria and damaged cells) and PREVENT cancer or make the body a less hospitable place for fast dividing, glucose guzzling cells.
Eating correctly means that our cells respond correctly to the signals and chemical cues of all other cells and tissues. Overfeeding and eating the worng things such as high carbs all the time disrupt this communication network and individual cells take over. With a constant surplus of the wrong nutrients individual cells take on the struggle for survival leading to conditions that favour overgrowth and therefore cancer.
My offices are squeezed between a Cancer research Institute and a high tech cancer treatment centre which is very busy every day. I hear the research (conventionally geared towards unrevelling the minutiae of the genetic mechanisms) and see the patients arrive to receive treatment from my window day in and day out. Not a pretty sight.
A young colleague who survived colon cancer told me that the nurses on the chemo ward would go around with candy and sweets for the patients….in the light of cancer as a metabolic disorder I cannot think of anything worse you could do for a cancer patient. Also a lot of the liquid foods they give patients during chemo are sugar loaded to give them energy. The offical NHS advice for cancer patients who suffer nausea and cachexia is to eat rich cakes and chocolate bars to secure calories especially for those who are losing weight…can you believe it??
SOmething’s gotta change. We must have gotten something terribly wrong. It is as if will the detail we know we are not looking at the bigger picture.
Sombrely yours
Paleofast
I very happy to learn that science is making the correct turn towards finding out the causes of cancer regardless does the finding benefit the big pharma or not.